

As of Jan. 17, veterans thinking about hurting themselves can get free crisis care, including inpatient, for up to 90 days at Veterans Affairs. They do not need to be enrolled in VA care. For immediate help, dial 988, then press 1.
Editor’s Note: This is the second story in a multipart series. Read the first story.
Army Sgt. Maj. Thomas Campbell didn’t intend to live long enough to make it to Afghanistan with the 182nd Infantry Regiment, a National Guard unit out of Massachusetts.
Campbell, a career infantryman in the Army, returned from Iraq in 2009 to an ended 20-year marriage and orders to head to the Sergeants Major Academy at Fort Bliss, Texas.
“When I get down to Fort Bliss, I’m by myself, I’m not busy, nobody’s in charge of me,” Campbell says. “I’m not in charge of anybody else—and I started to self-medicate.”

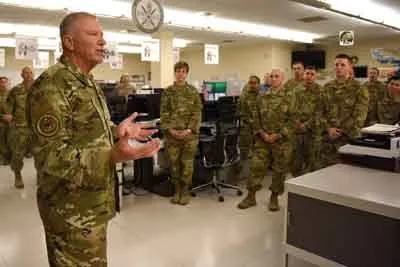
Command Sgt. Maj. Thomas E. Campbell, the outgoing senior enlisted adviser for 188th Infantry Brigade, 1st Army Division East, smiles during his farewell speech at a change-of-responsibility ceremony Sept. 30, 2020, at Fort Stewart, Georgia. Photo by Spc. Jose Escamilla, courtesy of the U.S. Army.
Campbell, who suffered mental and physical pain—in part, he says, from traumatic brain injuries during previous Iraq and Afghanistan deployments—rehearsed his own death: an accidental drive off a cliff on a Texas road with a tricky turn. The Army would not list his death as suicide, and that’s the way he wanted it.
“I don’t know how many times I rehearsed it, so when it came down to the execution, it would be flawless,” he says. “I had to get my affairs in order before I executed my suicide so my kids would get the benefits.”
The day he didn’t want to rehearse anymore, he rode his motorcycle up the road only to find a car parked at the spot. An interruption. And then he received a phone call from his girlfriend. Another interruption. He didn’t pick up. She called again. Another interruption. That one saved his life.
“To this day, I cannot remember the conversation,” Campbell says. His girlfriend—now wife—had no idea she was intervening. “It’s not what she said, it’s a matter of, she said something.”
Exactly a year later, Campbell headed to Afghanistan as part of the provincial reconstruction team in Kunar, to which the 182nd’s Delta Company, second platoon, a Massachusetts National Guard unit, was attached. After he returned in 2012, Campbell sat on review boards for more than 70 suicides across the active Army.
By then, he better understood what had happened to him, and that normal responses to war can transfer to peacetime life in a negative way. He knew maintaining connections—connections who can “interrupt” when things feel dire—could save lives. He knew the National Guard needed help to deal with the challenges of sending recently deployed soldiers back to civilian jobs, families, and lives, usually without the resources that come from daily interactions with others who have had similar experiences—or from the resources allotted to active-duty soldiers. And as National Guardsmen deploy more often in response to fires, floods, storms, and civil unrest, he knew the solution wouldn’t come with the end of the forever wars.
‘A Separation Solution to an Attachment Problem’
People kill themselves because they feel they no longer belong, psychologist and leading suicide expert Thomas Joiner says. The sense of social connection is so important to well-being that “thwarted belongingness” and “perceived burdensomeness”—a person no longer feels accepted and that they are a burden to others—is a precursor to considering suicide.
Brain images show stark changes in the way the amygdala—the emotional response portion of the brain—communicates with the front part of the brain in people who are at increased risk to kill themselves. Those brain patterns can change a person’s behavior, even if it’s not obvious to the people around them.
“It’s more difficult to do emotion regulation and to self-regulate and to do the things that help you lead a healthy life,” says Dr. Gregory Fricchione, associate chief of psychiatry at Massachusetts General Hospital.
Besides its capacity to process emotions, the amygdala also connects to the parts of the brain tied to physical pain and the area most responsible for making decisions, as well as another part of the brain that holds memory. Our brain’s triangular relationship between emotions, decisions, and pain suggests we mainly make decisions to minimize pain—and sometimes memories trigger pain and anxiety.

U.S. Navy sailors assigned to the aircraft carrier USS John C. Stennis distribute pamphlets to raise awareness for suicide prevention in Newport News, Virginia, Sep. 30, 2021. Photo by Mass Communication Spc. 2nd Class Thomas Pittman, courtesy of the U.S. Navy.
As many as 44 veterans die by suicide in the United States per day, which is 2.4 times higher than Veterans Affairs’ reported national suicide rate, according to a 2022 report by the nonprofit suicide prevention group America’s Warrior Partnership, which gathered data about veteran deaths from eight states, including Massachusetts. Since 2011, nearly a dozen soldiers who deployed to Afghanistan with the two Massachusetts National Guard infantry units have killed themselves.
But people aren’t programmed to hurt themselves, Joiner says. Humans instinctively fear death and actively try to escape threatening situations. The military also trains service members to survive. Self-harm, then, must be something learned, something that builds over time. And some service members experience a more gradual decline than others, with deaths occurring years after they were exposed to trauma.
“One of the primary steps involved in where people become suicidal is where they feel less and less connected to the people around them that they should be connected to,” Fricchione says. “That isolation part, whether it’s self-inflicted or not, is a huge factor.”
Soldiers may take different paths to die by suicide, which makes it difficult to get a handle on it. But they have at least one thing in common, Fricchione says:
“Suicide comes at a point of exasperation where you have given up on ever finding secure attachment,” Fricchione says. “It’s a separation solution to an attachment problem.
“So when you think about the problem in the military, you have to think about all the variations on that common theme,” he says. “It’s enormous.”
‘The Key to Our Survival’
For centuries, the amygdala—the part of the brain that processes emotions like fear, pleasure, and anger—has evolved to reward the body for feeling settled into the people and places around it.
“We’re all bound up in that need to feel attached and socially accepted,” Friccione says. “[It] becomes the key to our survival.”
When a person feels strong emotions, such as threatened or scared, the amygdala amps up, releasing a chemical that triggers feelings of anxiety. On the battlefield, a hypercharged amygdala can keep a service member alert and see them safely through an attack.
But threats that prompt an amygdala response don’t have to be physical. The brain also perceives separation, or loss of attachment, as a threat, Fricchione says. So when a soldier comes home, reintegration can feel like walking off a sharp cliff after an intense period of attachment to others. Combat ignites the body’s chemical responses—and so does a life synchronized with others in every way, from fighting together to eating together to sleeping in the same room or ditch.
“You had a jazzed-up brain for a long period of time,” Fricchione says. “That creates a very vivid memory track and embellishes the sense of need for attachment. And you come back and suddenly it’s like somebody turned off the lights.”
There’s no longer the need to keep watch at all hours of the night. No need to run on adrenaline. No enemy eyes on you. No need to react fast or fiercely.
“All the stress hormones crash when you get home because you don’t have the external stress to keep them elevated,” says Kenneth Pitts, the 182nd’s deployment operations sergeant major. He’s now a research psychologist at the U.S. Army Research Institute for the Behavioral and Social Sciences at Fort Benning, Georgia, where he studies biological responses to war-induced traumatic stress.
Award-Winning Journalism in Your Inbox
The deployed body, used to operating on high levels of adrenaline and stress hormones like cortisol, grapples with how to respond as the brain works to silence those signals when service members return home.
“Now you have low energy, you’ve got a harder time focusing, it’s harder for you to pull your thoughts out to find the right words to process complex things,” Pitts says. “There’s a higher tendency to do avoidance behaviors where, instead of engaging with problems and getting into the details to figure it out, you tend to distance yourself from problems and just turn it into a fuzzy stressful blob and not really deal with it.”
As combat veterans reflect and ruminate, some may interpret otherwise normal events—like gatherings with friends or family, or quick encounters with strangers—negatively, even if they’re not, Pitts says.
And the environment a service member returns to can emphasize and even enable negative thoughts, feelings, and behaviors.
“The physiological reinforcements, the cognitive reinforcements, the behavioral reinforcements—the three of these lines trend together in putting the person into the frame of mind that’s ripe for some of these extreme solutions to these problems,” Pitts says. “Perhaps they’re exaggerating some of [their problems], perhaps they’re developing a narrative that only leaves them one way out or limited ways out.”
To counter these changes, some combat veterans seek out the high of another deployment as an antidote to the biological crash. It can add meaning that feels as if it’s missing when a person goes from being a soldier trying to rout Taliban to a computer salesman or a student. But at some point, repeated deployments become an unsustainable avoidance method, and service members must reckon with change head-on.
‘It Was Easier Over There’
Col. Eric DiNoto’s deployment to Afghanistan almost immediately followed his first deployment to Iraq—and issues that began in Iraq ballooned in Afghanistan, he says. DiNoto served, as a major, as the executive officer for the 182nd during the 2011 Afghanistan deployment.
“A lot from the first deployment came up after that second deployment,” he says.
His disassociation from life at home to focus on the mission abroad turned to depression and dependency when he returned, he says.
“It’s weird because there’s almost sometimes—you feel awful for thinking it—but you think that it was easier when you’re over there,” he says.
He wasn’t the only one who faced difficulties coming home. For some, detachment became a mechanism to cope, but it only made things worse. For some soldiers, avoidance brought alcohol and drug dependency, aggression, and paranoia.
“You get more stressed out about those things and start to generalize that stress to other things in your life, too,” Pitts says.

Adam Markel, the CEO at More Love Media Group, speaks to U.S. Marines with the I Marine Expeditionary Force Information Group at Marine Corps Camp Pendleton, California, Oct. 8, 2021. Marines attending the resiliency boot camp learn about the importance of resiliency and how to use new skills. Photo by Cpl. Andrew Skiver, courtesy of the U.S. Marine Corps.
Service members need to be taught how to reacclimate—even if they feel as if they haven’t changed, Pitts says. A strong reintegration program could help soldiers better adjust to life after deployment.
“The majority tends to habituate—they get fine and they come back and they get reintegrated back home—and most people just kind of adapt without issue,” Pitts says. “So for people that don’t, it’s very challenging to figure out how their individual characteristics, whether that be environmental or driven by personality, all contributed to this negative trending.”
Some service members find it difficult to undo what their bodies and brains have settled into during prolonged periods of intensity. In a war zone, those habits—hypervigilance, a constant flow of adrenaline, always waiting for the worst to happen—keep people alive. At home, those “maladaptive habits”—what Pitts calls negative learning—can take hold as soon as the first 90 days of their return and could last as long as a lifetime.
After 9/11, the traditional culture, structure, and support systems couldn’t keep up with the changing pace of the Guard, says retired Brig. Gen. Jack Hammond, who oversaw the 181st and 182nd Infantry Regiments’ Afghanistan deployments as brigade commander of the 26th Yankee Division.
“The challenge was, when they came home, there was no care in place to support them,” Hammond says. He became the executive director of the Massachusetts-based veterans’ clinical program Home Base, which provides care for veterans and their families, after he returned home.
Annual data released by the Defense Department parses suicide deaths between the Guard and active components, but there are limited studies comparing each to understand the factors that contribute to suicide deaths. But Hammond, who spent a large part of his 31-year career on active duty assigned to the Guard, says the disparities in support for the Guard compared to the active component have become more blatant in recent years.
“For the Guard, their challenge is they live in the private world,” Hammond says.
Most National Guardsmen have full-time civilian sector jobs and don’t live on a military base—or anywhere near one. That means the robust community support networks and even physical proximity to other military families found on military bases simply don’t exist.
The dual commitment to a military and civilian career has also presented a unique challenge in recent years, Pitts says.
“As you go up in the ranks and your responsibilities mount, you have another career that’s happening between [activations] that’s doing the same thing,” Pitts says. “In between deployments, they’re trying to squeeze in all that productivity to make up for their absence, to get their careers and goals back on track so that timeline isn’t affected as much.”
National Guard soldiers also only have access to military health treatment centers when they’re on active-duty status. For most, that’s about 38 days a year.
And seeking out civilian care adds an extra layer of difficulty: Civilian health care workers are less likely to have training in either military culture or combat-related post-traumatic stress disorder. This means that not only do clinicians not understand when a soldier says, “I got blown up,” or, “We were always searching for IEDs outside the FOB,” but they may not be properly trained to address issues like moral injury or to listen to stories that may be traumatizing in a way they’re not used to.
Even seemingly small slip-ups are enough to turn off a veteran on edge. One soldier who served with the 182nd says he didn’t return to a therapist who asked him to recall his experiences in Iran. He served in Afghanistan.
Multiple Guard members say they had sized up clinicians and decided they didn’t want to work with experts who didn’t have some connection to the military—regardless of their expertise in the field. Knowing this, combat veterans make up the majority of Command Sgt. Maj. William Davidson’s outreach team at Home Base, and members of the family outreach team are all military-connected. Davidson, who served with the 181st during the 2011-2012 deployment, now is the director of veteran outreach and peer support at Home Base.
Chaplain Maj. Gen. Steven Schaick, U.S. Air Force chief of chaplains, visited the Combined Air Operations Center at Al Udeid Air Base, Qatar, Nov. 7, 2019. He spoke to airmen about the importance of being resilient in a deployed location and how resilience supports readiness and builds a more lethal force. Photo by Senior Airman Hope Geiger, courtesy of the U.S. Air Force.
Fricchione, who also works as a clinician for Home Base, has experienced questions of credibility firsthand, he says.
“When somebody like me—and I’ve never fought a war—I say, ‘Well, I think you should take this medicine,’ or ‘I think you should try this therapy,’ they say, ‘F you, you don’t know what you’re talking about. You didn’t really experience it,’” he says.
“There’s no arguing with the authenticity remark or critique of people who haven’t been through it themselves,” he says. “It’s hard to compete with that.”
But that rationale poses yet another challenge for service members: getting out of their own ways.
“That’s a big problem,” Fricchione says. “I don’t think anybody’s really solved that.”
‘It’s OK to Get Help’
DiNoto first received care at Home Base the summer after the battalion returned from Afghanistan. Motivated by his family, he stuck with formalized care at Home Base—off and on initially, and then steadily for two years, he says.
DiNoto also relied on outside veterans-based groups that focus on strengthening connections.
“I just made sure that it was consistent, even when I didn’t think I needed it,” he says.
Evidence-based care for veterans has expanded since the start of the post-9/11 wars. Mental health clinicians at VA and hospital-affiliated clinical programs like Home Base use specialized cognitive behavioral therapy for veterans, which may include exposing them to stress-inducing objects, thoughts, or memories to help desensitize them. Some clinical programs also incorporate psychedelics, such as MDMA and ketamine, as experimental therapies to address thoughts of suicide.
Stewart, who initially struggled with the stigma associated with treatment—that his soldiers would think he was “weak,” or that future employers, including within the military, might associate “care” with “dysfunction”—eventually sought military-provided services until he retired. Other service members, like DiNoto, who also acknowledged the stigma, instead turned to programs outside the Guard, so the Army has no record of it at all.

Marines with Marine Corps Support Facility New Orleans watch a resiliency training video between events during a field exercise at Camp Villere, Slidell, Louisiana, March 12, 2020. After each event, squad troop handlers discussed critical topics, such as suicide prevention and sexual assault. Photo by Lance Cpl. Leslie Alcaraz, courtesy of the U.S. Marine Corps.
The National Guard has tried to address the high number of suicides at the unit level. At nearly every drill, trained ambassadors and behavioral health workers teach service members how to help themselves or others. Sometimes, retired service members talk about the care they’ve received, Davidson says. But units struggle to find current peers willing to talk about their own care because they fear it will harm their careers.
“That’s what we need,” Davidson says. “We need senior leaders or other soldiers saying, ‘It’s OK to get help, and we’re still in.’”
Service members are more likely to seek care if other members who have undergone similar experiences encourage them, Fricchione says. That can be much stronger than encouragement from even close family members.
“That is a plus, and it’s also a minus, because they’re shutting out so many people who they don’t consider to be credible or authentic,” Fricchione says.
Retired Col. John Rodolico says he felt that way while he served in Iraq as an executive officer of a combat stress medical company, overseeing medical teams that debriefed units after traumatic events.
“If I’m coming into an infantry unit, and I’m a psychologist, and I’m doing one of these debriefings, I’ve got to really sell myself on these guys, especially after a traumatic event,” he says.
His team trained the infantry unit leaders to lead the conversations. When one of their own conducted the debriefs, the soldiers were more likely to engage, he says.
“The closer the person leading these groups is to the identity of the unit, the better,” he says. “They were more successful.”
Rodolico also served as deputy commander for the Massachusetts National Guard’s medical command, overseeing response efforts following the initial suicide deaths in the state’s two infantry battalions.
But there’s yet another barrier: the belief that there aren’t enough clinical resources to get help even if a person seeks it out.
“We have a lot of training on how to identify [a struggling soldier], how to help a friend, how to take them when they’re really at their lowest to the VA, or to a provider for help,” says one soldier who served with the 182nd and wanted to remain anonymous. In training and war, a “battle buddy” constantly ensures their partner is safe. The military has worked to carry that model to mental health by having battle buddies watch for signs of distress.
“What frustrates me is when [the] battle buddy did everything he could,” the soldier says. “He even identified it. He even was brave enough to go take him and convince him that he needs to go check in. Then, literally within a week of doing that, they still kill themselves.
“We don’t get enough help.”
Care in the Guard relies heavily on service members’ accounts of their own mental health. The Guard’s annual Unit Risk Inventory survey includes questions about a service member’s personal well-being to help their leadership identify high-risk thoughts and behaviors.
After a deployment, the military requires service members to take two surveys that assess their returning experience—once at their demobilization station, and another at least 90 days after they return home. The surveys are meant to capture any reported struggles, but behavioral health experts in the Massachusetts National Guard say data is limited to what a service member wants to disclose.
In recent years, the National Guard has centralized its behavioral health and wellness programs under one division, called Warrior Resilience & Fitness. Since 2014, the Massachusetts Guard’s behavioral health team has grown from one person to five full-time clinicians. Some of the program’s voluntary initiatives emphasize fitness groups to help maintain connection among service members, as well as nutrition and other aspects of self-care.
“Human beings have autonomy, and we can provide all of these services, and if somebody doesn’t want to engage in them, or doesn’t want to share what’s going on. … ” says Maj. Katherine Murphy, director of warrior resilience and fitness with the Massachusetts National Guard. “We’re still seeing that they make those choices and take their lives.”

Capt. Anthony Priest, behavior health officer with 1st Signal Brigade, speaks with Company B, 304th Expeditionary Signal Battalion-Enhanced, about mental health issues July 26, 2022. Photo courtesy of the U.S. Army.
The Massachusetts National Guard has partnered with a few groups to help Guard members build resilience. But they’re not clinical-standard prevention and intervention methods, and active-duty guardsmen are much more likely to participate than the one-weekend-a-month guys, soldiers told The War Horse.
Though the Guard informally offers, after a deployment ends, 90 transition days before soldiers return to drill, there’s no scientifically defined period for the body and brain to acclimate, especially as they continue to navigate a foot in both worlds, Fricchione says. The process can last for the remainder of a service member’s military career—or beyond.
Within 30 days of the end of a deployment, military leaders encourage soldiers and their families to attend a yellow-ribbon reintegration program, and soldiers must meet with a mental health specialist. The specialists pair soldiers identified as at-risk with a psychological health coordinator to connect the soldiers to resources, Murphy says. These post-deployment events have stayed the same since well before the 182nd’s 2011 deployment.
“We all struggle [with] how do we meet folks where they’re at, so they are in a place of comfort to let us know that they are struggling,” Murphy says. “And that looks different, feels different for every single human being on this Earth.”
‘We Do Preventive Maintenance on Everything Else’
Like substance abuse disorder or most cancers where an individual is forever regarded as remaining in recovery or remission, resilience requires continual maintenance. Mental health treatment can be normalized just like other tangible methods of upkeep in the military, but not if it remains voluntary, Hammond says.
“We do preventive maintenance for everything in the military from day one,” he says.
Driving a Humvee requires maintenance and service checks before and after use, as does using a weapon. Mental health care should be treated the same way, Hammond says.
“We do it a little bit now while they’re there with behavioral health teams, and on the back end [of a deployment] we ask them if they’re OK,” Hammond says. “It should be a presumptive condition that they require some transition on the way out.”
But just as not every Humvee needs an oil change or a tightened lug nut, the solutions can’t be the same for each soldier, he says.
“We have these outliers that find a well of resilience and lead extraordinary lives, but we also know there are versions of terminal illness in psychiatry where people are so wounded that we don’t feel good about their chances,” Fricchione says. “But nowadays, there’s more and more hope.”

All military mental health programs are geared toward suicide prevention and increasing resiliency, according to military public affairs. The military also offers unit-based resiliency training, stress- and anger-management training, outpatient counseling services, family advocacy, and alcohol and drug abuse counseling. Photo by Joshua J. Seybert, courtesy of the U.S. Air Force.
Some bring childhood trauma or an internalized negative mindset with them into service. Others may be working through a moral injury—either participating in or witnessing an atrocity that defies personal values. Some endure an identity crisis as they transition out of the military and struggle to define who they are without it. Some experience a combination of some or all.
In some cases, a soldier may be managing fine, but adding another major stressor—a breakup, a lost job, the death of a friend—can be enough to push that person into crisis.
Service members who have deployed are more likely to report higher levels of depression, anxiety, and stress compared to those who haven’t, but several studies suggest that the type, length, or even the number of deployments is not a sole indicator of suicide risk.
But while the number of combat deployments have decreased for Guardsmen, their suicide rates have not. And as they increasingly deploy in response to natural and manmade disasters— such as forest fires and floods, as well as civil unrest, such as that seen in Washington, D.C., after the Jan. 6, 2021 attacks—their experiences remain extreme. They’ve had to adapt to those new, often traumatic situations, as well.
“Often, [soldiers] don’t really know how they’re adapting,” Pitts says. “How they’re paying attention to information differently, how they’re putting themselves in the mindset to get a better night’s sleep, how they’re able to compartmentalize different types of stress.”
There are obvious, fixable problems, Guard members told The War Horse. For one, not everyone is a risk, but everyone receives constant training, which takes millions of dollars in resources away from those who could use some extra help. The Defense Department has spent $100 million on research alone, according to the Rand Corporation.
Some evidence-based programs don’t involve seeing a clinician or any form of medical intervention. They instead offer opportunities for veterans to reflect on their physical and emotional health and make meaningful connections with other service members. Veterans of earlier wars once found that sense of belonging in a VFW lounge; now, they may be more likely to find it in veteran groups that offer everything from equine therapy to rafting, hiking, and camping.
In fact the solution, the soldiers and therapists seemed to agree, is ancient.
Over generations, the Army has perfected the art of forming unit-based bonds. During training, soldiers go through intentionally stressful situations not only to strengthen individual readiness, but to build trust and unit cohesion through shared experience.
“The success of the Army, and the success of the individuals in these battalions, is going to depend on that social attachment,” Fricchione says.
With so much time spent together under different levels of duress, a syncing occurs among service members—a harmonizing of emotions, behavior, and perhaps even physiological responses, Fricchione says. The more time spent and experiences shared, the stronger the bonds.
Our Journalism Depends on Your Support
Legend tells us this bond transcends life. According to Norse mythology, the bravest half of warriors who die in combat are promised a seat in the god Odin’s hall of slain warriors, known as Valhalla. The goddess Freyja takes the other half—the ordinary warriors—to the field of warriors. In Valhalla, warriors gather to fight during the day and feast at night, preparing for the end of the world when they’ll be called upon to assist Odin, the god of war and death, in the ultimate battle at the world’s end. Though intended only for those who die in combat, “Til Valhalla”—until we meet again in Valhalla—is written and said for any service member who has died, regardless of how.
The phrase has taken on a deeper scientific meaning to many who have grappled with suicide prevention in the ranks. To some, it validates that social attachment—a symbol of strength and resilience—is promised to the warrior, if not during the end stages of life, then eternally in death. Even those who die by suicide die on a recognizable battlefield, slain by a familiar enemy and worthy to their comrades of a seat in Valhalla.
For those working in suicide prevention, it is also a call to act—to create an environment that maintains strong bonds and renews attachments; to help soldiers feel that life, too, is a worthy place to live.
Maybe Valhalla can wait.
This War Horse investigation was reported by Lara Salahi, edited by Kelly Kennedy, fact-checked by Ben Kalin, and copy-edited by Mitchell Hansen-Dewar. Headlines are by Abbie Bennett. Maria Wilson contributed to this report.

Jesus Christ is King

Comments are closed.